
 French
French Deutsch
DeutschSchwannoma
| Schwannoma | |
|---|---|
| Other names | neurilemoma,[1]: 621 neuroma,[2] neurolemoma,[2] Schwann cell tumor[2] |
 | |
| Micrograph of a schwannoma showing both a cellular Antoni A area (top) and a loose paucicellular Antoni B area (bottom). HE stain. | |
| Specialty | Neuro-oncology |
A schwannoma (or neurilemmoma) is a usually benign nerve sheath tumor composed of Schwann cells, which normally produce the insulating myelin sheath covering peripheral nerves.
Schwannomas are homogeneous tumors, consisting only of Schwann cells. The tumor cells always stay on the outside of the nerve, but the tumor itself may either push the nerve aside and/or up against a bony structure (thereby possibly causing damage). Schwannomas are relatively slow-growing. For reasons not yet understood, schwannomas are mostly benign and less than 1% become malignant, degenerating into a form of cancer known as neurofibrosarcoma. These masses are generally contained within a capsule, so surgical removal is often successful.[3]
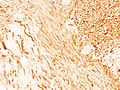
Schwannomas can be associated with neurofibromatosis type II, which may be due to a loss-of-function mutation in the protein merlin.[4] They are universally S-100 positive, which is a marker for cells of neural crest cell origin.
Schwannomas of the head and neck are a fairly common occurrence and can be found incidentally in 3–4% of patients at autopsy.[4] Most common of these is a vestibular schwannoma, a tumor of the vestibulocochlear nerve that may lead to tinnitus and hearing loss on the affected side. Outside the cranial nerves, schwannomas may present on the flexor surfaces of the limbs. Rare occurrences of these tumors in the penis have been documented in the literature.[5]
Verocay bodies are seen histologically in schwannomas.
Variants
[edit]- Pleural schwannoma is extremely rare. A unique subtype of schwannoma that typically develops in superficial (cutaneous or subcutaneous) sites and may be identified by its development pattern, which is plexiform (intraneuralnodular).[6][7] The correlation with schwannoma predisposition disorders like NF2 and schwannomatosis, however, is minimal (approximately 5 percent of cases).[8] These tumors might lack a capsule or be less encapsulated than a typical schwannoma.More challenging to identify from MPNST are the infrequent plexiform schwannomas that develop in deep anatomical sites, such as soft tissue[9] or major peripheral nerves.[10] These tumors may exhibit enhanced cellularity and mitotic activity. Although the likelihood of these tumors developing into cancer is extremely low, local recurrence is possible in around half of cases. On MRI, it usually shows hyper or iso-intensity on T1-weighted images and heterogenous hyperintensities on T2 weighted images. Pleural schwannoma typically shows fatty degeneration, hemorrhage, perivascular hyalinization, and cystic formation thus giving heterogenous hyperintensities on T2 weighted images. Complete surgical removal of pleural schwannoma is the usual treatment.[11]
- Cellular schwannoma is a relatively rare variation. Cellular schwannoma is nearly exclusively made up of a fascicular proliferation of well-differentiated Schwann cells that are cytologically bland, missing Verocay bodies, and just slightly exhibiting Antoni B pattern growth (10% of the tumor area).[12][13][14] Local recurrence is Variable (5-40%) and perhaps greater than in normal schwannomas.[15][16]
- Malignant melanotic nerve sheath tumor (previously known as melanotic schwannoma) is a rare aggressive peripheral nerve sheath tumor that typically develops in conjunction with spinal or visceral autonomic nerves, consisting uniformly of Schwann cells displaying melanocytic differentiation. About half of the cases are associated with Carney complex.[17]
Gallery
[edit]-

-

-
 Subcutaneous schwannoma
Subcutaneous schwannoma -
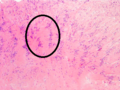 Antoni A area of schwannoma with Verocay bodies (one annotated by circle)
Antoni A area of schwannoma with Verocay bodies (one annotated by circle) -

-

-

.JPG)
_Antoni_B.jpg)

_Antoni_B.jpg)
_Antoni_B.jpg)
_S-100_immunostain.jpg)
See also
[edit]- Intranodal palisaded myofibroblastoma
- List of inclusion bodies that aid in diagnosis of cutaneous conditions
- Neurofibroma
- Palisaded encapsulated neuroma
References
[edit]- ^ James WD, Berger T, Elston D (2006). Andrews' diseases of the skin : clinical dermatology (10th ed.). Philadelphia: Saunders Elsevier. ISBN 978-0-7216-2921-6.
- ^ a b c Rapini RP, Bolognia JL, Jorizzo JL (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- ^ Biswas D, Marnane CN, Mal R, Baldwin D (September 2007). "Extracranial head and neck schwannomas--a 10-year review". Auris, Nasus, Larynx. 34 (3): 353–359. doi:10.1016/j.anl.2007.01.006. PMID 17376620.
- ^ a b Hanemann CO, Evans DG (December 2006). "News on the genetics, epidemiology, medical care and translational research of Schwannomas". Journal of Neurology. 253 (12): 1533–1541. doi:10.1007/s00415-006-0347-0. PMID 17219030. S2CID 11854280.
- ^ Nguyen AH, Smith ML, Maranda EL, Punnen S (June 2016). "Clinical Features and Treatment of Penile Schwannoma: A Systematic Review". Clinical Genitourinary Cancer. 14 (3): 198–202. doi:10.1016/j.clgc.2015.12.018. PMID 26797586.
- ^ Fletcher CD, Davies SE. Benign plexiform (multinodular) schwannoma: a rare tumour unassociated with neurofibromatosis. Histopathology. 1986; 10:971–980. [PubMed: 3096870]
- ^ Woodruff JM, Marshall ML, Godwin TA, Funkhouser JW, Thompson NJ, Erlandson RA. Plexiform (multinodular) schwannoma. A tumor simulating the plexiform neurofibroma. Am J Surg Pathol. 1983; 7:691–697. [PubMed: 6638259]
- ^ Berg JC, Scheithauer BW, Spinner RJ, Allen CM, Koutlas IG. Plexiform schwannoma: a clinicopathologic overview with emphasis on the head and neck region. Hum Pathol. 2008; 39:633–640. [PubMed: 18439936]
- ^ Agaram, N. P.; Prakash, S.; Antonescu, C. R.; "Deep-seated plexiform schwannoma: a pathologic study of 16 cases and comparative analysis with the superficial variety", American Journal of Clinical Pathology, 29:1042–1048, 2005 [PubMed: 16006798]
- ^ Hebert-Blouin MN, Amrami KK, Scheithauer BW, Spinner RJ. Multinodular/plexiform (multifascicular) schwannomas of major peripheral nerves: an underrecognized part of the spectrum of schwannomas. J Neurosurg. 2010; 112:372–382. [PubMed: 19499977]
- ^ Iwasaki T (2016). "Giant ancient schwannoma of the pleura: Commentary". Lung India. 33 (4): 449–50. doi:10.4103/0970-2113.184928. PMC 4948239. PMID 27578944.
- ^ Casadei GP, Scheithauer BW, Hirose T, Manfrini M, Van Houton C, Wood MB. Cellular schwannoma. A clinicopathologic, DNA flow cytometric, and proliferation marker study of 70 patients. Cancer. 1995; 75:1109–1119. [PubMed: 7850709]
- ^ Fletcher CD, Davies SE, McKee PH. Cellular schwannoma: a distinct pseudosarcomatous entity. Histopathology. 1987; 11:21–35. [PubMed: 3557324]
- ^ Wick, M. R.; Swanson, P. E.; Scheithauer, B. W.; Manivel, J. C.; "Malignant peripheral nerve sheath tumor: An immunohistochemical study of 62 cases", American Journal of Clinical Pathology, 87:425–433, 1987 [PubMed:2435144]
- ^ White W, Shiu MH, Rosenblum MK, Erlandson RA, Woodruff JM. Cellular schwannoma. A clinicopathologic study of 57 patients and 58 tumors. Cancer. 1990; 66:1266–1275. [PubMed:2400975]
- ^ Casadei GP, Scheithauer BW, Hirose T, Manfrini M, Van Houton C, Wood MB. Cellular schwannoma. A clinicopathologic, DNA flow cytometric, and proliferation marker study of 70 patients. Cancer. 1995; 75:1109–1119. [PubMed: 7850709]
- ^ Yeom, Jeong A; Song, You Seon; Lee, In Sook; Han, In Ho; Choi, Kyung Un (2022-08-26). "Malignant melanotic nerve sheath tumors in the spinal canal of psammomatous and non-psammomatous type: Two case reports". World Journal of Clinical Cases. 10 (24): 8735–8741. doi:10.12998/wjcc.v10.i24.8735. ISSN 2307-8960. PMC 9453363. PMID 36157803.
External links
[edit]| Authority control databases: National |
|---|